

Nicoll A, Danielsson N.. A novel reassortant avian influenza A(H7N9) virus in China – what are the implications for Europe. Euro Surveill. 2013;18(15):pii=20452.
As of 10 April 2013, 33 human cases infected with a novel influenza A(H7N9) virus have been laboratory confirmed in Shanghai, Anhui, Jiangsu and Zhejiang provinces in China (Figure1). This case count came after on 31 March 2013, the Chinese authorities had announced the identification of a novel influenza A virus, an A(H7H9) virus, in three people in Shanghai and Anhui province. Two men in Shanghai, 87 and 27 years old, respectively, had become ill with influenza-like (ILI) symptoms and progressed to severe lower respiratory tract infections within a week in mid to late February, and died from acute respiratory distress syndrome hereafter [1,2]. The two had no epidemiological link and no known exposure to evidently sick animals. One of them was a pork butcher. The third case was a 35-year-old woman from Anhui province, adjacent to Shanghai, who also became ill with ILI with symptom onset on 9 March followed by severe respiratory disease and death.
Figure 1. Laboratory-confirmed influenza A(H7N9) cases in China as of 10 April 2013 (n=33)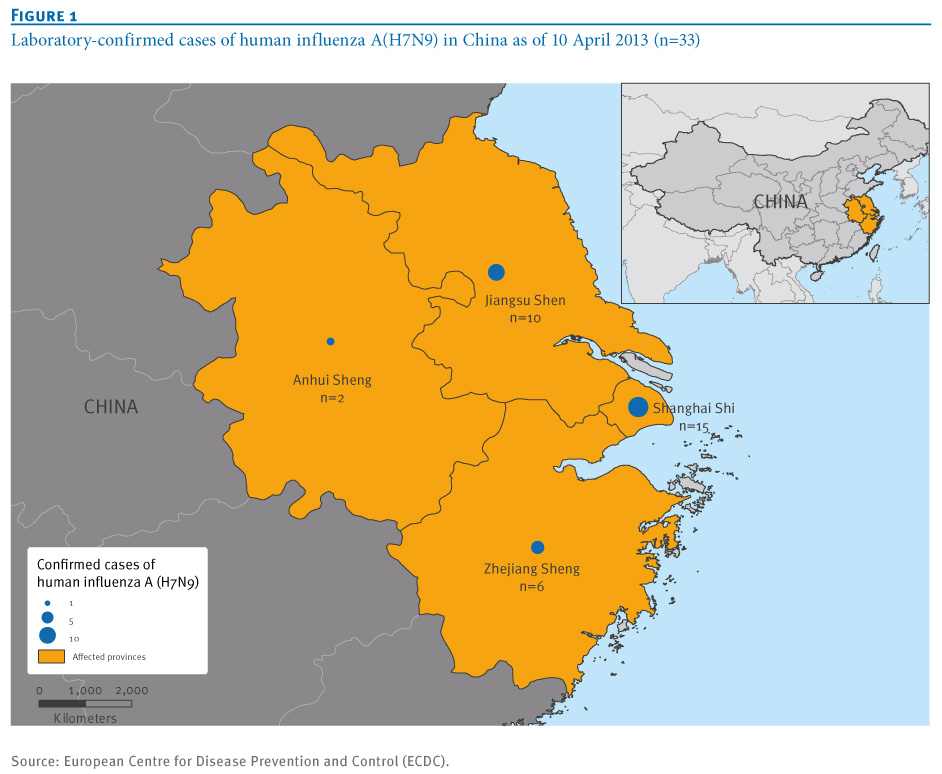
The detection of these cases was possible because of a well-functioning surveillance system with a laboratory component through which the initially non-subtypeable influenza A viruses were sent to the World Health Organization (WHO) Influenza Collaborating Centre at the Chinese Center for Disease Control and Prevention (CDC) in Beijing for sequencing. Upon laboratory identification of the new viruses, the responsible Chinese authorities notified the cases as required in the International Health Regulations (IHR) to WHO and other member states [3].
Moreover, researchers from the Chinese CDC posted the genetic information of the viruses on the publicly accessible GISAID website [4]. The viruses were not genetically identical, indicating they had been circulating for some time over a wide region [5]. The same type of viruses were reported by Chinese veterinary authorities from 4 April onward in different species of poultry and environmental samples from live bird markets in Shanghai [6]. The sequences of the veterinary and environmental specimens were also posted on the GISAID site by the Chinese national veterinary laboratory in Harbin [3].
Following the detection of the first cases, the Chinese CDC has rapidly made specific polymerase chain reaction (PCR) test kits for the new A(H7N9) viruses available to provincial and local laboratories across China to ensure timely testing of suspected cases. Since then individual human cases are being confirmed and made public daily by the Chinese authorities at provincial level in the four affected provinces. More cases are being detected with onset dates since late March (Figure 2). While this could simply reflect increasing awareness among clinicians and public health authorities and that testing became available more widely, close monitoring is necessary to detect changes in transmission patterns, especially human-to-human transmission and cases appearing in China beyond the four provinces.
While the novel A(H7N9) virus has been detected in birds and environmental specimens at a bird markets in Shanghai and the other affected provinces, the source of infection in most of the cases still remains to be determined [6 ]. It is equally unclear how the virus is introduced into the markets. Nevertheless, China has stepped up vigilance and intensified human and animal surveillance [7]. It has also implemented public health measures that include the closure of some live poultry and bird markets and culling of birds [8].
A striking feature is that human cases are sporadic and very few possible clusters have been detected. They are being investigated by the Chinese authorities. So far, there has been no documented sustained human-to-human transmission and there is no clear indication of such transmission even though the virus has genetic markers that are known to be associated with improved replication of avian influenza viruses in mammals [4,5].
When compared with A(H5N1) viruses, animal-to-human transmissibility seems to be higher for influenza A(H7N9). It is noteworthy that the timeframe during which cases have been identified is very different from that of human cases of influenza A(H5N1) detected in China of late. Between January 2010 and March 2013, only seven human A(H5N1) cases were reported, five of which are known to have died [9]. Few human cases due to infection with avian influenza A(H7) viruses have been described in the literature, possibly because the symptoms are usually mild in humans and of low pathogenicity in poultry [10]. A well described outbreak involving humans was that of a highly pathogenic avian influenza A(H7N7) among poultry in the Netherlands in 2003. It resulted in 86 mild infections, mainly conjunctivitis, among poultry workers, three cases of non-sustained human-to-human transmission among their household contacts, but only one fatality [11,12].
Only careful serological surveys in China can reveal if there were such transmissions and these investigations are underway. Of the detected 33 human A(H7N9) cases as of 10 April, 30 developed severe illness with nine fatalities while three presented with mild symptoms (Figure 2). It can be expected that surveillance activities will lead to detection of additional cases in the coming weeks, but so far no cases have been identified outside the four Chinese Provinces.
Figure 2. Laboratory-confirmed cases of human influenza A(H7N9) by week of symptom onset and severity as of 10 April, China March- April 2013 (n=30) 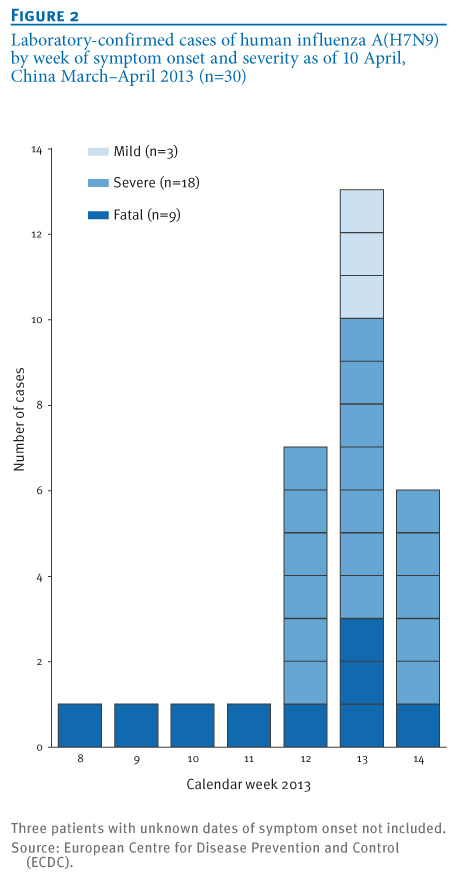
A limited number of scenarios that could follow from the emergence of this novel virus are possible. The one that explains the current human and animal epidemiological situation best, based on available clinical and virological analyses, is that of the emergence of a novel reassortant avian influenza virus of low pathogenicity to birds but of significant pathogenicity to humans. This virus has probably spread undetected among poultry in parts of eastern China. When this started is unclear. It only came to light because some people infected through contact with birds or environmental exposure, became severely ill. Even though the viruses were found in poultry and the environment in live bird markets in Shanghai, the species introducing the infection into the markets has not been identified. The various species reported as being infected may have only become infected at the markets.
The speed, transparency and intensity of the work performed in respect to the novel A(H7N9) virus in China and by the Chinese CDC and veterinary authorities is impressive and deserves full credit [13]. It also has to be acknowledged that there is tremendous value for all those concerned with public health in that the WHO Collaborating Centre for Influenza at the Chinese Center for Disease Control and Prevention has shared the viruses and that the molecular data have been published on the publicly accessible GISAID database. This data sharing platform has been important for scientists to gain important insight into the molecular virus characteristics and the origins of the virus as well as for public health experts to assess the current situation.
However, the tasks lying ahead, namely analysing, describing and especially controlling the virus cannot be underestimated. The extent of distribution of this A(H7N9) virus in domestic poultry in China and possibly other countries is unclear and surveillance and control of a low pathogenicity avian influenza virus in countries with complex mixes of informal and formal poultry sectors will be challenging. The markers of poultry die-offs seen with high pathogenicity avian influenza A viruses such as H5N1 and H7N7, will not signal the presence of the new A(H7N9) virus. In such situations, animal surveillance on the basis of sampling of live birds, including wild birds, such as done in Hong Kong and in European Union (EU) countries will be essential [14,15].
What are the possible implications of the current situation for Europe and European citizens and which actions should the EU take and which ones have been taken already? The European Centre for Disease Prevention and Control (ECDC) published its first risk assessment on 3 April and is providing updated assessments and short reports on the epidemiology as new information emerges [16]. Several guidance documents on prevention of infections, infection control and case management developed earlier for influenza A(H1N5) by ECDC, WHO and Member States are, with some modifications, applicable to the current situation [16-18]. Visitors to China and other countries where avian influenzas have caused severe human disease of late [9], should avoid visiting bird markets and follow basic hygienic measures. Persons returning from China who develop severe respiratory infection within 10 days should be evaluated and tested for the new virus to rule out such infection [17], though most likely another infection will be detected. Case management and infection control guidelines for A(H5N1) apply in the short term. This will include antiviral treatment given that the Chinese CDC promptly established that the A(H7N9)viruses are susceptible to neuraminidase inhibitors [4,5].
There is a standing procedure in place in Europe to send all non-subtypeable influenza A viruses isolated from humans promptly to the WHO Collaborating Center in London for further analysis. Notwithstanding this, ECDC, the WHO Regional Office for Europe, the WHO Influenza Collaborating Centre, the University of Bonn and the Community Network Reference Laboratories are working in together to make testing for A(H7N9) possible in all National Influenza Centres in Europe as soon as possible.
Some candidate H7 and H9 vaccines viruses already exist under WHO’s strain selection system for the eventuality of an emerging virus [19]. They may not be effective against the new influenza A(H7N9) virus and once the regulatory laboratories have obtained the novel virus, WHO and presumably EU authorities will now need to consider if they wish to proceed with the very early stages of vaccine development as has been done for the candidate H7 and H9 viruses.
Overall, how concerned Europe should be cannot yet be determined. The new virus is a reassortant virus based on an haemaglutinin antigen A(H7) to which most humans will not have been exposed. Therefore, if human-to-human transmission starts, and that is only an ‘if’, population immunity cannot be presumed. It would have to be assessed now by determining age-specific sero-reactivity of human sera to this influenza A(H7N9) virus as a priority. Immunity, or lack of it, in the human population are key data required for assessing pandemic risk. As stated above, they needed to come from field investigations in China as well as seroepidemiological studies in Europe based on protocols developed precisely for such situations [20].
At this very moment it cannot be ruled out that there are some human-to-human transmissions causing mild or asymptomatic infections as happened in the Netherlands in 2003. It also remains unclear to what extent the predominance of severe disease may represent a bias because mainly people with severe disease are tested. Investigations of patients’ contacts including serological studies, will clarify this point. Such investigations orchestrated by the Chinese CDC are underway.
There will be many other calls for research and it will be important and difficult to prioritise. Fortunately a framework exists for making decisions on priorities. The Influenza Risk Assessment Tool (IRAT) has been developed since 2011 for this purpose by the United States (US) Centers for Disease Control and Prevention with some international partners [21,22]. It looks at 10 parameters bundled into three families: properties of the virus, attributes of the population, ecology and epidemiology. It has already been deployed to inform US decisions on the A(H3N2)v vaccines. It does not predict pandemic risk or make decisions but it informs decisions. Though the IRAT is still being evaluated as a tool it will certainly indicate what should be some of the most important public health research priorities for A(H7N9).
It is also important that the sequence and virological analyses are considered in combination with the epidemiological findings. Despite the virological markers described in the recent report from the WHO Collaborating Centres [5] it should not be seen as inevitable on the longer term that this reassortant A(H7N9) will develop efficient human-to-human transmissibility or become established in Europe, though both should be kept in mind as possibilities. Neither has happened for the highly pathogenic influenza A(H5N1) virus in the decade and a half since its emergence in China in 1996 [23]. Despite multiple detections of the A(H5N1)virus in wild birds and some outbreaks in domestic poultry flocks in Europe, the high levels of biosafety in the EU have not permitted A(H5N1) viruses to become established in European domestic poultry. It is fortunate that the European Commission and the Member States have since 2007 established surveillance for low pathogenicity avian influenza in domestic and wild birds in Europe [14]. The recent events have underlined the importance of this system.
Acknowledgements
The authors acknowledge that some of these analyses have been possible using the virological and genetic molecular data provided in the publicly accessible GISAID database by the WHO Collaborating Centre for Influenza at the Chinese Center for Disease Control and Prevention.
References
- Chinese Center for Disease Control and Prevention (CDC). Questions and Answers about human infection with A(H7N9) avian influenza virus. Beijing: CDC; 31 Mar 2013. Available from: http://www.chinacdc.cn/en/ne/201303/t20130331_79282.html
- World Health Organization (WHO). Global Alert and Response (GAR). Disease Outbreak News. Human infection with influenza A(H7N9) virus in China. Geneva: WHO; 1 Apr 2013. Available from: http://www.who.int/csr/don/2013_04_01/en/index.html
- World Health Organization (WHO). International Health Regulations 2005 second edition. Geneva: WHO; 2008. Available from: http://whqlibdoc.who.int/publications/2008/9789241580410_eng.pdf
- Global Initiative on Sharing All Influenza Data (GISAID). GISAID EpiFlu Database. USA: GISAID Foundation. [Accessed 10 Apr 2013]. Available from: http://platform.gisaid.org/epi3/frontend#307300
- World Health Organization Regional Office for Europe (WHO/Europe). Public health relevant virological features of Influenza A(H7N9) causing human infection in China. Copenhagen: WHO/Europe. 2013. Available from: http://www.euro.who.int/__data/assets/pdf_file/0008/186677/050413-H7N9-influenza-viruses-Virologic-features_update.pdf
- World Organisation for Animal Health (OIE). Low pathogenic avian influenza (poultry), China (People´s Rep. of). Paris: OIE. [Accessed 10 Apr 2013]. Available from: http://www.oie.int/wahis_2/public/wahid.php/Reviewreport/Review?page_refer=MapFullEventReport&reportid=13238
- Food and Agriculture Organization of the United Nations (FAO). Strong biosecurity measures required in response to influenza A(H7N9) virus. Rome: FAO; 5 Apr 2013. Available from: http://www.fao.org/news/story/en/item/173655/icode/
- European Centre for Disease Prevention and Control (ECDC). Epidemiological update of 11 April: novel influenza A virus A(H7N9) in China. Stockholm: ECDC; 11 Apr 2013. Available from: http://www.ecdc.europa.eu/en/press/news/Lists/News/ECDC_DispForm.aspx?List=32e43ee8-e230-4424-a783-85742124029a&ID=888&RootFolder=%2Fen%2Fpress%2Fnews%2FLists%2FNews
- World Health Organization (WHO). Cumulative number of confirmed human cases for avian influenza A(H5N1) reported to WHO. Geneva: WHO; Mar 2013. Available from: http://www.who.int/influenza/human_animal_interface/H5N1_cumulative_table_archives/en/
- Belser JA, Bridges CB, Katz JM, Tumpey TM. Past, present, and possible future human infection with influenza virus A subtype H7. Emerg Infect Dis. 2009;15(6):859-65. http://dx.doi.org/10.3201/eid1506.090072. PMid:19523282. PMCid:2727350.
- Koopmans M, Wilbrink B, Conyn M, Natrop G, van der Nat H, Vennema H, et al. Transmission of H7N7 avian influenza A virus to human beings during a large outbreak in commercial poultry farms in the Netherlands. Lancet. 2004;363(9409):587-93. http://dx.doi.org/10.1016/S0140-6736(04)15589-X
- Du Ry van Beest Holle M, Meijer A, Koopmans M, de Jager CM. Human-to-human transmission of avian influenza A/H7N7, The Netherlands, 2003. Euro Surveill. 2005;10(12):pii=584. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=584. PMid:16371696.
- Heymann DL, Mackenzie JS, Peiris M. SARS legacy: outbreak reporting is expected and respected. Lancet. 2013;381(9869):779-81. http://dx.doi.org/10.1016/S0140-6736(13)60185-3
- Leung YH, Zhang LJ, Chow CK, Tsang CL, Ng CF, Wong CK, et al. Poultry drinking water used for avian influenza surveillance. Emerg Infect Dis. 2007;13(9):1380–2. http://dx.doi.org/10.3201/eid1309.070517. PMid:18252115. PMCid:2857302.
- European Commission (EC) DG Health and Consumers. Animals. Avian influenza. Surveillance. Surveillance for Health Influenza. Brussels: EC. Available from: http://ec.europa.eu/food/animal/diseases/controlmeasures/avian/eu_resp_surveillance_en.htm
- European Centre for Disease Prevention and Control (ECDC). Rapid risk assessment. Severe respiratory disease associated with a novel influenza A virus, A(H7N9) – China. Stockholm: ECDC; 3 Apr 2013. Available from: http://www.ecdc.europa.eu/en/publications/Publications/AH7N9-China-rapid-risk-assessment.pdf
- European Centre for Disease Prevention and Control (ECDC). Technical report. Avian influenza portfolio. Collected risk assessments, technical guidance to public health authorities and advice to the general public Stockholm, June 2006. Stockholm: ECDC. Jun 2006. Available from: http://ecdc.europa.eu/en/publications/Publications/0606_TER_Avian_Influenza_Portafolio.pdf
- World Health Organization (WHO). Influenza. Influenza at the Human-Animal Interface. Geneva: WHO. [Accessed 10 Apr 2013]. Available from: http://www.who.int/influenza/human_animal_interface/en/
- World Health Organization (WHO). Influenza. WHO recommended candidate viruses for vaccine development and production for the northern hemisphere 2013-2014 influenza season. All available candidate vaccine viruses and potency reagents. Geneva: WHO. [Accessed 10 Apr 2013]. http://www.who.int/influenza/vaccines/virus/candidates_reagents/home/en/
- Van Kerkhove MD, Broberg E, Engelhardt OG, Wood J, Nicoll A; The CONSISE steering committee. The consortium for the standardization of influenza seroepidemiology (CONSISE): a global partnership to standardize influenza seroepidemiology and develop influenza investigation protocols to inform public health policy. Influenza Other Respi Viruses. 2012. [Epub ahead of print].
- Trock SC, Burke SA, Cox NJ. Development of an influenza virologic risk assessment tool. Avian Dis. 2012;56(4 Suppl):1058-61. http://dx.doi.org/10.1637/10204-041412-ResNote.1. PMid:23402136.
- Centers for Disease Control and Prevention (CDC). Influenza Risk Assessment Tool (IRAT). Atlanta: CDC. Available from: http://www.cdc.gov/flu/pandemic-resources/tools/risk-assessment.htm
- World Health Organization (WHO). H5N1 avian influenza: Timeline of major events. Geneva: WHO; 17 Dec 2012. Available from: http://www.who.int/influenza/H5N1_avian_influenza_update_20121217b.pdf
See Also:
Latest articles in those days:
- Birth cohort effects in adults associated with influenza A(H1N1)pdm09 vaccine effectiveness 10 hours ago
- Genetic Characterization of Swine Influenza Viruses in Thailand in 2019-2025 Reveals Novel Reassortants 10 hours ago
- Outbreak dynamics of high pathogenicity avian influenza virus H5N1, clade 2.3.4.4b euBB, in black-headed gulls and common terns in Germany in 2023 11 hours ago
- [preprint]The canine respiratory epithelium is a permissive ecosystem for influenza interspecies transmission and emergence 11 hours ago
- [preprint]Explainable and Calibrated AI for Decoding Host-Adaptive Changes in Influenza A Virus 11 hours ago
[Go Top] [Close Window]