

Belgian working group on influenza A(H1N1)v.. Influenza A(H1N1)v virus infections in Belgium, May-June 2009. Euro Surveill. 2009;14(28):pii=19270
Introduction
On 25 April 2009, the World Health Organization (WHO) declared an outbreak of A(H1N1)v influenza, first reported by the United States (US) [1] and Mexico, a ’Public Health Event of International Concern‘ (PHEIC) under the International Health Regulations [2]. The WHO Director-General raised the pandemic alert phase to the maximum level (phase 6) on 11 June 2009 [3]. As of 14 July 2009, 30 of 31 European Union (EU) and European Free Trade Association (EFTA) countries have reported cases of influenza A( H1N1)v [4].
On 12 May 2009, the Belgian National Reference Laboratory for Influenza confirmed the first case of influenza A(H1N1)v in a person returning to Belgium from the US. A total of 130 confirmed cases have been detected in Belgium as of 14 July 2009.
An active surveillance system was implemented, following a delaying strategy. It aimed at detecting cases of A(H1N1)v influenza in travellers returning from affected areas [5] and in their contacts for the purpose of taking control measures to delay the spread of the virus.
Methods
Table 1 shows the case definitions developed for the investigation and the case classification used.
Table 1. Case definition and case classification for A(H1N1)v influenza, Belgium, May-June 2009
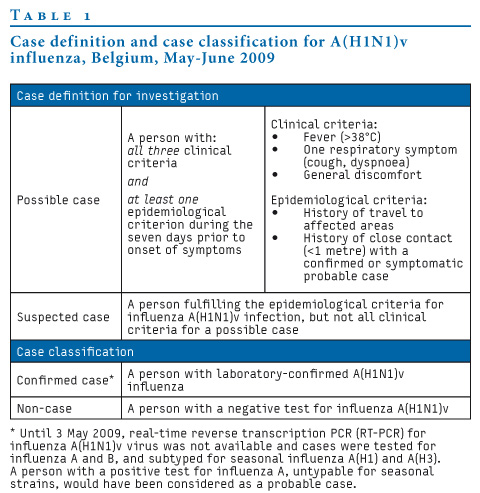
The Interministerial Influenza Coordination Committee disseminated protocols for case and contact management regarding notification, sampling, prophylaxis, treatment and isolation. The involved physicians, mostly general practitioners (GPs), were required to contact the Community Health Inspectorate when finding a possible or suspected case. Physicians took samples and sent them on the same day to the National Reference Laboratory for Influenza. Samples were treated under biosafety level 3 (BSL3) conditions and tested by realtime reverse transcription PCR (RT-PCR) using primers directed against A and B influenza virus, and in case of a positive result for A influenza also with primers against A(H1) and A(H3); from 3 May 2009 we also used primers specific for A(H1N1)v influenza virus, sent from the Centers for Disease Control and Prevention (CDC).
All involved public health authorities scaled up their response service to operate around the clock. A duty service with epidemiologists was available for Health Inspectorates and involved physicians through a restricted access telephone hotline in order to support them with case definitions and the organisation of sampling.
Hospitalisation was recommended for the first 25 confirmed cases for the purpose of isolation. From 2 June 2009 onwards, the recommendation was for patients to stay at home for seven days after onset of symptoms and to hospitalise severe cases only. Confirmed cases were treated with neuraminidase inhibitors.
Provincial health inspectorates performed contact tracing. Close contacts of confirmed cases should take a neuraminidase inhibitor as prophylaxis and were requested to stay at home for seven days after the latest contact and to avoid unnecessary further contacts as a quarantine measure. Close and other contacts were advised to seek immediate medical advice if they noticed fever or respiratory symptoms.
Cases were notified to the WHO and through the Early Warning and Response System (EWRS) to the European Centre for Disease Prevention and Control (ECDC) by the Belgian Federal Public Service for Public Health (FPS).
Results
As of 14 July, 633 people have been tested in Belgium and 130 cases of influenza A(H1N1)v have been confirmed. Two of the possible cases were not tested because they were close contacts of confirmed cases and under antiviral prophylaxis when they developed influenza symptoms.
We analysed the first 43 laboratory-confirmed cases. Infection was acquired abroad by 35 cases, of which 18 had a travel history to the US, nine had returned from the Dominican Republic and three from the United Kingdom (UK). The other imported cases had returned from Argentina (n=1), Australia (n=1), Canada (n=1), Chile (n=1) and Costa Rica (n=1). The first eight imported cases had come back from the US. Seven imported cases declared onset of symptoms prior to their return. According to information available for 26 of 28 cases, disease onset occurred up to five days after arrival (mean 1.6 days, median 2 days).
All indigenous cases (n=8) were close contacts to previously confirmed cases. Figure 1 shows the evolution of the cases by date of symptom onset and by import status.
Figure 1. Distribution of laboratory-confirmed cases of influenza A(H1N1)v by date of onset and by import status, Belgium, 12 May-28 June 2009 (n=43)
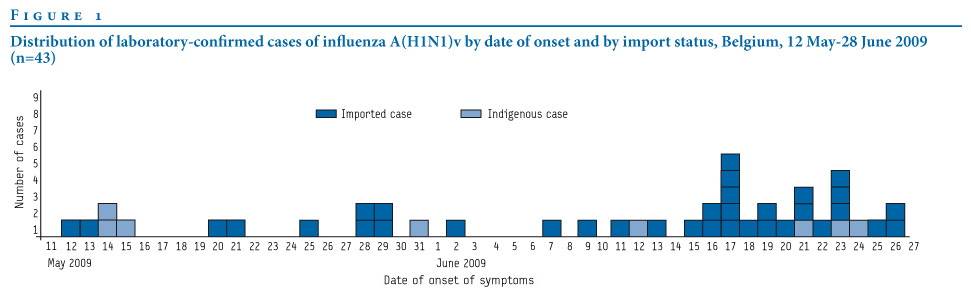
Table 2 shows the geographic distribution of the cases by province. On 28 June 2009, eight of 11 provinces in Belgium were affected. One third of the cases were residents in the province of Antwerp. One case who had been in transit at Brussels airport was counted in the province of Flemish Brabant.
Table 2. Distribution of laboratory-confirmed cases of influenza A(H1N1)v by province of residence, Belgium, 12 May-28 June 2009 (n=43)

The female to male ratio was 1.05 (22 women and 21 men). The age range was from eight months to 51 years (median: 28 years, mean: 29 years). Seven cases were younger than 20 years. The most affected age group were the 20-29 year-olds with 16 cases.
Figure 2. Distribution of cases of influenza A (H1N1)v by age group and import status, Belgium, 12 May-28 June 2009 (n=43)

Information about symptoms was available for 42 cases. The most commonly reported symptoms were cough in 40 cases followed by general discomfort in 38 cases and fever or history of fever in 36 cases. Dyspnoea was reported by 12 cases and diarrhoea by five cases; nausea was reported by two cases and vomiting, sore throat and headache were reported by one case each.
No complications have been detected so far. One confirmed case, already under treatment with oseltamivir, was hospitalised because influenza symptoms persisted and the patient had asthma as underlying condition. Respiratory samples from this patient are currently being cultured and tested for resistance against oseltamivir. One pregnant woman was confirmed to be infected with influenza A(H1N1)v. Information on underlying factors for the other 41 patients was not available.
Discussion
When Belgium detected the first confirmed case of influenza A(H1N1)v, many neighbouring countries had already notified cases. We assume that the number of Belgian travellers to Mexico is small compared to that of more populated European countries and that the number of Belgian travellers returning from the US is larger than the amount of those returning from Mexico. This may explain why Belgium started detecting imported cases when sustained community transmission happened in the US.
Continuous monitoring of affected areas worldwide and consequent updating of the case definition allowed the detection of cases returning from countries with a low number of cases but with evidence of community transmission like Costa Rica or the Dominican Republic.
The age distribution of the cases may reflect the age of the people that travel and is not representative of the Belgian population. Children of school age were only sporadically affected until 11 July 2009, and this may have played an important role in the disease not spreading in the community. Secondary cases occurred in the same age groups as imported ones, reflecting the importance of contact patterns. However, an outbreak in a summer language school that has affected 14 people between 10 and 18 years-old, is currently under investigation.
This preliminary analysis of the 43 first confirmed cases of influenza A(H1N1)v in Belgium suggests that the clinical manifestation resembles that of seasonal influenza. This is consistent with an analysis by the ECDC on aggregated data of European cases of influenza A(H1N1)v [6].
Currently, mitigation strategies are being adopted by countries in the southern hemisphere that are facing the influenza season, such as Chile, New Zealand and Australia, but also by European countries where sustained community transmission has been declared, like the UK [7]. In Belgium, the Interministerial Influenza Coordination Committee announced the switch to a mitigation strategy on 13 July 2009. This will require appropriate surveillance of influenza-like illness. A GP-based sentinel surveillance network for seasonal influenza is being reinforced in Belgium and from 14 July 2009 onwards has taken over the enhanced system put in place from the beginning of the pandemic. This network aims at characterising the circulating influenza viruses, seasonal or pandemic strain, as well as estimating the burden of disease at community level. The Belgian system for the monitoring of mortality will contribute to observing the situation.
Conclusions
The introduction of influenza A(HN1)v virus in Belgium happened in the same way as in other EU/EFTA countries, causing a small but increasing number of cases. Given the uncertainty of the evolution of the current influenza A(H1N1) pandemic, and the emergence of complications in a small proportion of the cases, the Belgian health authorities continue to closely monitor the severity and the spread of the disease in order to provide an adequate response during the coming months.
Working group:
The Belgian working group on influenza A(H1N1)v is formed by the Flemish Community, the French Community, the Brussels Region, the Hospital Saint-Pierre in Brussels and the Federal Public Service for Public Health under the coordination of the Interministerial Influenza Coordination Committee. The corresponding author is S.Quoilin, IPH (s.quoilin@iph.fgov.be).
References
- Centers for Disease Control and Prevention (CDC). Swine influenza A (H1N1) infection in two children – Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep. 2009;58(15):400-2.
- International Health Regulations (2005). 2nd ed. Geneva: World Health Organization; 2008. ISBN 978 92 4 158041 0. Available from: http://whqlibdoc.who.int/publications/2008/9789241580410_eng.pdf
- World now at the start of 2009 influenza pandemic. Statement to the press by WHO Director-General Dr Margaret Chan. Geneva: World Health Organization; 11 June 2009. Available from: http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html
- Influenza A(H1N1)v infection. ECDC situation reports on influenza A(H1N1)v. Stockholm: European Centre for Disease Prevention and Control; 13 July 2009. Available from: http://ecdc.europa.eu/en/files/pdf/Health_topics/Situation_Report_090713_1700hrs.pdf
- Scientific Institute of Public Health. Pays touchés par la grippe A/(H1N1)v [Countries affected by influenza A/(H1N1)v]. [In French]. 2005-2009 comité de coordination interministériel Influenza. [Accessed on 3 July 2009]. Available from: http://www.influenza.be/fr/H1N1_pays_fr.asp
- ECDC working group on influenza A(H1N1)v. Preliminary analysis of influenza A(H1N1)v individual and aggregated case reports from EU and EFTA countries. Euro Surveill. 2009;14(23):pii=19238. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19238
- Areas of widespread community transmission. London: Health Protection Agency. [Accessed on 3 July 2009].
See Also:
Latest articles in those days:
- Birth cohort effects in adults associated with influenza A(H1N1)pdm09 vaccine effectiveness 5 hours ago
- Genetic Characterization of Swine Influenza Viruses in Thailand in 2019-2025 Reveals Novel Reassortants 5 hours ago
- Outbreak dynamics of high pathogenicity avian influenza virus H5N1, clade 2.3.4.4b euBB, in black-headed gulls and common terns in Germany in 2023 6 hours ago
- [preprint]The canine respiratory epithelium is a permissive ecosystem for influenza interspecies transmission and emergence 6 hours ago
- [preprint]Explainable and Calibrated AI for Decoding Host-Adaptive Changes in Influenza A Virus 6 hours ago
[Go Top] [Close Window]