

Health Protection Agency West Midlands H1N1v Inves. Preliminary descriptive epidemiology of a large school outbreak of influenza A(H1N1)v in the West Midlands, United Kingdom, May 2009. Euro Surveill. 2009;14(27):pii=19264
Introduction
On 27 April 2009, the first two confirmed cases of the pandemic influenza A(H1N1)v in the United Kingdom (UK) were reported in Scotland. As of 2 July 2009 there have been 7,447 cases reported in the UK [1]. During the early phase of the outbreak, the majority of the cases were amongst travellers, initially those returning from Mexico and then also those returning from the United States (US). The first indigenously acquired case was reported on 1 May 2009 and since then an increasing number of indigenous cases have been reported [2].
Since the outbreak in the UK began, transmission has occurred in a number of school settings [3]. We present the results of a preliminary epidemiological investigation on an influenza A(H1N1)v outbreak that began in mid May in a primary school in Birmingham, West Midlands, England.
Epidemiological description of the outbreak
On 18 May 2009, the Health Protection Agency (HPA) was informed of an increased rate of absenteeism in a primary school in Birmingham, West Midlands. The school has 419 pupils in the primary school and 60 in a nursery and is located in inner city Birmingham, in the West Midlands region, England. Symptoms reported included fever, respiratory and gastrointestinal symptoms. None of the symptomatic pupils had a history of school absence for holiday travel in the seven days before onset of symptoms. On 19 May 2009, given that some symptoms described were influenza-like, nose and throat swabs were arranged for a small number of symptomatic pupils. One specimen was confirmed on 21 May by real-time PCR specific for influenza A(H1N1)v.
On 21 May, the school closed for seven days; this period coincided with a scheduled school holiday of one week. Between Saturday, 23 May and Monday, 25 May, the investigation team attempted to contact, by telephone, parents of pupils as well as members of staff on lists provided by the school in order to administer a brief questionnaire. Information collected included: demographic details, symptoms, recent travel history and details of out-of-school activities. Information about household and close social contacts was also recorded.
Upon conclusion of the telephone interview parents of all asymptomatic children were advised that their children should start a prophylactic course of antiviral medicine being distributed at the school on 23 and 24 May. A total of 304 asymptomatic children were prescribed prophylaxis. Parents of children who were symptomatic at the time of interview or who had been symptomatic in the previous seven days were asked to stay at home so that specimens (nose and throat swabs) could be collected from their child(ren). At the time of swabbing, all symptomatic children were provided with a treatment course of oseltamivir. Contact tracing was carried out to identify household contacts and close social contacts. The contacts were then followed up by an out-of-hours general practitioner (GP) service and provided with antiviral prophylaxis.
All pupils and staff attending the primary school were contacted. Of 563 pupils/members of staff, 175 (31%) were symptomatic and required testing. Of those 175, 64 (37%) were found to be positive for influenza A(H1N1)v. A further 139 symptomatic household contacts were tested out of 664 identified. Household contacts are excluded from the data analysis, and analysis is restricted to only laboratory confirmed cases.
Figure 1 shows the date of symptom onset for cases of influenza A(H1N1)v in the school. Of the 64 cases, 31 (48%) reported symptom onset between 18 and 21 May. At the time of interview and before treatment had started, symptoms reported by the 64 confirmed cases included: subjective fever (54, [84%]); nasal congestion (45 [70%]) and sore throat (38 [59%]) (Table 1). No cases were hospitalised and the duration of illness was not recorded.
Figure 1. Confirmed cases of influenza A(H1N1)v among pupils and staff by date of illness onset, school outbreak West Midlands, May 2009 (n=64)
Table 1. Symptoms reported by influenza A(H1N1)v cases among pupils and staff, school outbreak West Midlands, May 2009 (n=64 confirmed cases*)
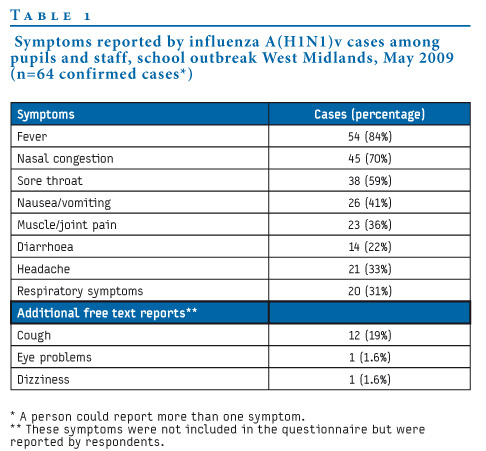
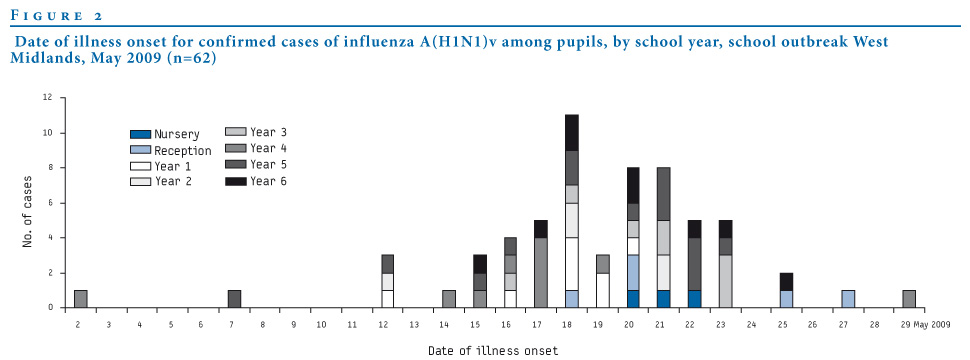
Table 2 shows the attack rate by school year group. The index case was confirmed on 21 May, but the earliest reported date of onset was 2 May (see Figure 2) in a year 4 pupil (aged nine years). The next date of onset was 7 May in a year 5 pupil (aged 11 years). Neither of these early cases had a travel history or history of contact with a confirmed case. Fifty-three percent of cases were female and the highest attack rate was seen in pupils in year group 5 (23%). Excluding two members of staff, cases ranged in age from 4 to 12 years, with a mean of 8.5 years and a median of 9 years. None of the cases had a recent history of travel outside the UK.
Table 2. Proportion of influenza A(H1N1)v cases among pupils in each school year and attack rate by year group school outbreak West Midlands, May 2009 (n=62 confirmed cases)
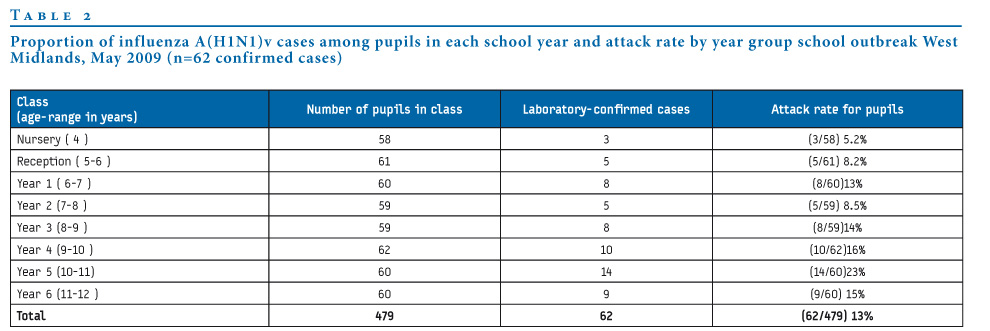
Figure 2. Date of illness onset for confirmed cases of influenza A(H1N1)v among pupils, by school year, school outbreak West Midlands, May 2009 (n=62)
Discussion and conclusion
A total of 64 confirmed cases of influenza A(H1N1)v have been identified in pupils and members of staff in a school in the Midlands, UK. This large primary school outbreak resulted in an overall clinical attack rate of 30% and a microbiologically confirmed attack rate of nearly 13%. The clinical attack rate in this single school is higher than the average attack rate of 24% reported for outbreaks of seasonal influenza in UK schools during the 2005-6 influenza season [4].
Feedback from interviewers and the GP out-of-hours service suggested that symptoms were generally mild in children, predominantly fever, nasal congestion and sore throat consistent with other case series from the UK reported thus far [3]. No children were hospitalised and no data were available on the duration of illness or on underlying disease in the cases. Most cases reported date of onset of symptoms between 18 and 21 May, suggesting that that the rate of transmission may have been highest during the period immediately prior to the school closing, when high absenteeism had been reported. The latest date of onset was 29th May, and most cases were asymptomatic by the time the school re-opened after the holidays on 1 June.
Subsequent to this incident, there have been no further cases in the school. However, cases continue to be identified in the local area with an increasing number of local schools reporting high absenteeism and confirmed cases. Cases occurring outside schools suggest ongoing and widespread community transmission in the area.
Further investigation of this school incident includes sequential swabbing of a subset of families with confirmed cases and presentation of data on those pupils who were symptomatic but were not laboratory-confirmed cases. These analyses will be presented at a later date.
Acknowledgements
The authors would like to thank the head teacher and staff of the school for providing the contact information for staff, pupils, the members of the West Midlands Flu Response Centre who completed the telephone interviews and the ‘Badger’ Team who undertook the collection of nose and throat swabs and the administration of antivirals.
Health Protection Agency West Midlands H1N1v Investigation Team:
Adedoyin Awofisayo, Gillian Smith, Babatunde Olowokure, Yasmin Rehman, Huda Mohammed, Harsh Duggal, Kulsum Janmohamed, Valerie de Souza, Fay Wilson, Sue Ibbotson, Mike Catchpole, Husam Osman, Erasmus Smit, Nick Phin, John Watson, Stephen Palmer, Richard Pebody, J Ellis, A Bermingham, and Maria Zambon, on behalf of all those in the HPA who are contributing to the ongoing investigation and management of the current influenza A(H1N1)v pandemic.
References
- Health Protection Agency (HPA). Update on swine flu cases 2 July 2009. [Accessed 9 July 2009]. Available from: http://www.hpa.org.uk/web/HPAweb&HPAwebStandard/HPAweb_C/1246519358678
- Health Protection Agency (HPA). HPA Weekly National Influenza Report 24 June 2009 (Week 26). [Accessed 29 June 2009]. Available from: http://www.hpa.org.uk/web/HPAwebFile/HPAweb_C/1245581558905
- Health Protection Agency and Health Protection Scotland new influenza A (H1N1) investigation teams. Epidemiology of new influenza A (H1N1) in the United Kingdom, April - May 2009. Euro Surveill. 2009;14(19):pii=19213. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19213
- Zhao H, Joseph CA, Phin N. Outbreaks of influenza and influenza-like illness in schools in England and Wales, 2005/06. Euro Surveill. 2007;12(5):pii=705.
See Also:
Latest articles in those days:
- Birth cohort effects in adults associated with influenza A(H1N1)pdm09 vaccine effectiveness 5 hours ago
- Genetic Characterization of Swine Influenza Viruses in Thailand in 2019-2025 Reveals Novel Reassortants 5 hours ago
- Outbreak dynamics of high pathogenicity avian influenza virus H5N1, clade 2.3.4.4b euBB, in black-headed gulls and common terns in Germany in 2023 6 hours ago
- [preprint]The canine respiratory epithelium is a permissive ecosystem for influenza interspecies transmission and emergence 6 hours ago
- [preprint]Explainable and Calibrated AI for Decoding Host-Adaptive Changes in Influenza A Virus 6 hours ago
[Go Top] [Close Window]