

Hahné S, Donker T, Meijer A, Timen A, van Steenber. Epidemiology and control of influenza A(H1N1)v in the Netherlands: the first 115 cases. Euro Surveill. 2009;14(27):pii=19267
Introduction
The first human infections with the new influenza A(H1N1) variant virus [A(H1N1)v], a novel triple reassortant swine influenza virus, were diagnosed in two patients in the United States on 14 and 17 April 2009 [1]. Subsequently, this virus was identified as the cause of a large, ongoing epidemic of respiratory disease in Mexico [2]. Following the report of community transmission in more than two regions, the World Health Organization (WHO) declared on 11 June 2009 the outbreak of influenza A(H1N1)v to be a pandemic [3]. In this short report we summarise the infection control and surveillance activities undertaken in the Netherlands in response to the emergence of influenza A(H1N1)v, as well as the epidemiological characteristics of the first 115 laboratory confirmed cases.
Infection control and case finding
In response to the emergence of the new, potentially pandemic, A(H1N1)v strain of influenza virus, the Centre for Infectious Disease Control of the National Institute for Public Health and the Environment (RIVM) in the Netherlands advised on 25 April that individuals who developed fever within seven days after returning from Mexico should consult their general practitioner (GP) by telephone. On 29 April, new influenza A(H1N1)v virus infection was upgraded to a Category A notifiable disease, requiring doctors and laboratories to report the name of the patient to the Municipal Health Service when the disease was suspected or identified. Notifications are entered by Municipal Health Services into a national anonymous web-based database, including information on travel history, contact with symptomatic cases and clinical symptoms. Enhanced surveillance was carried out for clusters and for suspected patient-to-healthcare worker transmissions.
The case definitions (Table) were based on the European Union case definitions [4].
Table. Case definitions for new influenza A(H1N1)v [4]
Indigenous cases were defined as cases with no history of travel abroad during the incubation period. In this report we only include laboratory-confirmed cases. Case finding was carried out by Municipal Health Services, who set out to offer laboratory testing to all reported possible cases of A(H1N1)v from 29 April onwards. Case finding was enhanced by testing all household and other close contacts of confirmed cases. From 28 May travellers with fever within seven days of arriving from the United States were also advised to consult their GP. As of 23 June, contacts (even if symptomatic) are no longer required to be tested for A(H1N1)v, unless this is indicated for their clinical management.
To control the spread of infection and attenuate disease in those infected, oseltamivir treatment was recommended from 30 April onwards for all possible, probable and confirmed cases, and for their contacts, irrespective of symptoms. This included airplane passengers seated in the same row as the index case as well as those in the two rows in front and behind. Infected individuals were advised to stay indoors for at least 10 days after the date of onset or shorter if laboratory testing turned negative after day five. The national pandemic influenza preparedness plan includes detailed instructions for protective equipment for health care workers [5]. Entry screening at airports, school closure and hospitalisation for infection control purposes have not been employed.
As of 23 June, asymptomatic contacts of confirmed cases are no longer recommended to receive oseltamivir. However, symptomatic contacts of laboratory-confirmed cases are still recommended to be treated with oseltamivir, and they continue to be notifiable.
Laboratory methods
Laboratory testing is carried out by the National Influenza Centre in the Netherlands (represented by Erasmus Medical Centre, Rotterdam and RIVM, Bilthoven) using general influenza A and A(H1N1)v specific real-time RT-PCR, initially with confirmation by sequence analysis [6]. Results of laboratory testing have been available within 32 hours after sampling to allow timely oseltamivir treatment and prophylaxis.
Methods to estimate key epidemiological parameters
For all indigenous cases we tried to identify a most probable source by examining the patients’ contact history reported by Municipal Health Services who interviewed cases. For all epidemiologically linked cases, we subsequently estimated the generation interval as the average number of days between the dates of symptom onset in the source case and in the secondary case.
To estimate the effective reproduction number (Re), we divided the epidemiological curve in windows of duration equal to the estimated generation interval. For each pair of successive windows in the period from 30 May to 18 June we calculated the ratio between the number of indigenous cases in one window and the total number of cases in the previous window. Re was then estimated by the average of this ratio.
Results
Incidence and travel history
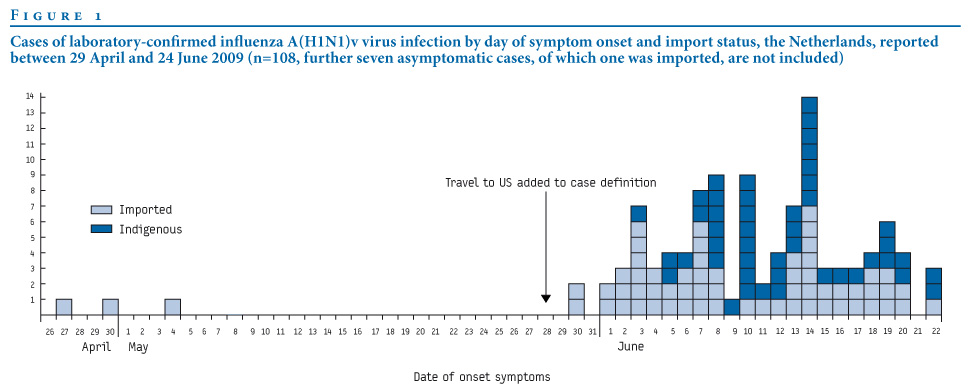
On 30 April the first laboratory-confirmed case of A(H1N1)v in the Netherlands was reported in a three-year-old girl who on 27 April returned with her parents from a family visit in Mexico. By 24 June, 115 confirmed cases were reported, of whom 64 (56%) were most likely imported and 51 (44%) were indigenously acquired (Figure 1). Three of the indigenous cases were in individuals who had not been in contact with any known case or cluster. These sporadic cases were tested for the new influenza A(H1N1)v virus because they presented with influenza-like illness (n=2) or viral pneumonia (n=1). So far, no cases of influenza A(H1N1)v have been detected in the sentinel influenza surveillance.
Figure 1. Cases of laboratory-confirmed influenza A(H1N1)v virus infection by day of symptom onset and import status, the Netherlands, reported between 29 April and 24 June 2009 (n=108, further seven asymptomatic cases, of which one was imported, are not included).
Clinical picture and vaccination status
None of the 115 reported confirmed cases has died. Two (2%) have been admitted to hospital, including a previously physically fit man who required admission to an intensive care department with severe viral pneumonia. He was tested for influenza A(H1N1)v after presenting with respiratory failure. He had not been in contact with any known cases, and had not travelled during the incubation period. The other hospital admission concerned a tourist with asthma visiting the Netherlands. She presented with influenza-like symptoms, and did not have pneumonia. She was admitted for social indications, and was discharged after less than 24 hours. One further case had clinically diagnosed pneumonia but was not admitted to hospital. Of all cases for whom information was available (n=46), three (7%) had underlying chronic illnesses. No cases in pregnant women have been reported.
Of the 48 indigenous, non-sporadic cases, six (13%) were asymptomatic at the time of sampling. It is yet unknown, however, whether they became symptomatic after sampling. Symptoms reported by laboratory-confirmed, symptomatic cases for whom this information was available included: sore throat, cough and/or coryza (93 cases, 90%), fever >=38?C (76 cases, 88%), myalgia (54 cases, 52%) and diarrhoea (9 cases, 9%).
Of 111 cases for whom the seasonal influenza vaccination status for 2008-9 was known, 17 (15%, 95% CI 9-23%) reported to have been vaccinated. In 2007, an estimated 10% of the practice populations of less than 65 years of age of GPs participating to a research network (LINH, the National Information Network of General Practice) were vaccinated, whilst 15% were targeted for vaccination [7]. In our case-series, 7% of cases below 65 years of age were in the target group for seasonal influenza vaccination due to underlying illnesses (see above), and only two cases were 65 years or older. The relatively high vaccine coverage among cases compared to the coverage among the general population is consistent with a lack of effectiveness of the 2008-9 seasonal influenza vaccine against the new influenza A(H1N1)v [8].
Epidemiological characteristics
Indigenous cases were younger than imported cases, with a median age of 18 and 31 years, respectively (p<0.05, Figure 2). Cases occurred in most Municipal Health Service regions, with three main clusters of indigenous transmission (Figure 3).
Figure 2. Cases of laboratory-confirmed influenza A(H1N1)v by age group and import status, the Netherlands, 29 April – 24 June 2009 (n=115)
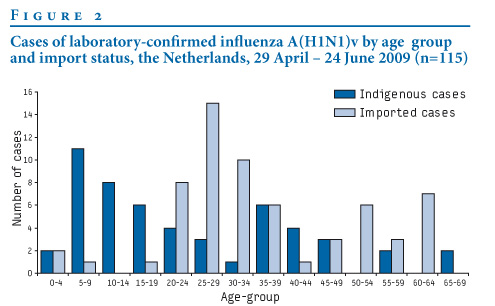
Figure 3. Cases of laboratory-confirmed influenza A(H1N1)v by Municipal Health Service region, the Netherlands, 29 April – 24 June 2009 (n=115)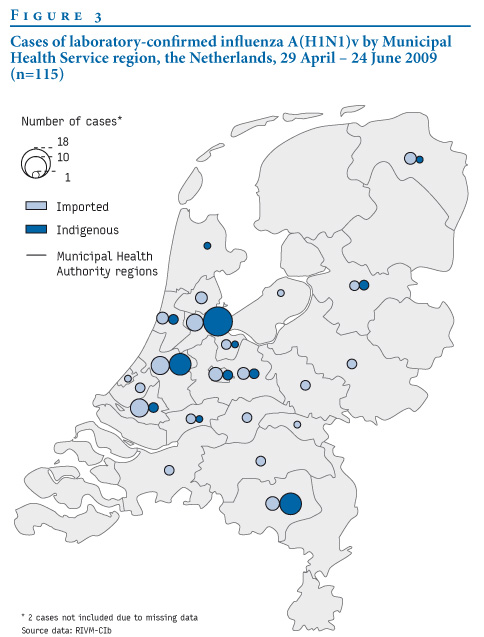
Of the 51 indigenous cases, 36 cases could be epidemiologically linked to an index case, 12 cases could be linked to a cluster and three cases were sporadic. Of four indigenous cases in healthcare workers who did not report contact with a case outside of work, one was considered as resulting from patient to healthcare worker transmission.
In total, nine clusters of more than one case were identified, including three larger clusters with 19, 12 and 9 cases, respectively. The mean generation (or serial) interval for these clusters was 2.5 days (standard deviation (SD) 0.9 days, cluster of 19 cases, n=13), 3.1 days (SD 1.1 days, cluster of 12 cases, n=8) and 2.8 days (SD 1.7 days, cluster of 9 cases, n=5). Overall, the generation interval was 2.7 days (SD 1.1, N=32).
Based on this, we applied a generation interval of three days as moving average window to the epidemic curve. The mean ratio of the number of indigenous cases in one window to the total number of cases in the previous window (the effective reproductive number Re) was 0.5 between 30 May and 18 June. We did not include cases with a date of onset after 18 June as due to the reporting delay we may have missed cases in this period, which would have resulted in an underestimation of Re. We observed that no epidemiological links could be traced back to the seven asymptomatic cases, suggesting a very low Re for asymptomatic cases. However, due to the small number of indigenous cases, the confidence bounds on these estimates of Re can be considered to be very wide. The implicitly assumed delta distribution gives an upward bias in the point estimate of Re. However, as the SD of the generation interval was small relative to the doubling time of the epidemic, this bias is negligible [9].
Conclusions
Despite repeated introductions of the new influenza A(H1N1)v into the Netherlands, our enhanced surveillance results suggest that indigenous transmission of this virus has remained relatively limited. A large proportion of cases were imported, and only 15% of these caused secondary cases. Moreover, only three clusters of more than four cases were detected, all relatively limited in size. This suggests that the Re was below one, consistent with our estimate of Re based on the epidemiological curve. Our point estimate of Re for the influenza A(H1N1)v epidemic in the Netherlands was lower than the R0 estimated for Mexico or the US [10]. However, as the number of indigenous cases was low, this point estimate needs to be considered cautiously. The estimated Re was based on observations in the period 30 May and 18 June, and is likely to change in future months. Explanations for the relatively low Re estimate may include the rigorous case-finding and infection control implemented in the Netherlands following the introductions of the influenza A(H1N1)v virus. However, our data do not allow drawing conclusions on the effectiveness of this policy. Our observations are consistent with an absence of effectiveness of the 2008-9 seasonal influenza vaccine against the current pandemic strain.
The incidence of reported cases of influenza A(H1N1)v in the Netherlands is much lower than in the United Kingdom [11]. This may reflect the phase of epidemic; the epidemic in the UK could be more advanced due to earlier and more frequent introductions, especially from the US. It may also reflect chance effects early on in the epidemic, where introductions into schools are likely to lead to intense transmission.
The clinical picture and severity of disease among our cases is similar to what was reported elsewhere [12]. However, due to the limited time of follow-up, we may have somewhat underestimated the severity in our report.
The occurrence of a new strain of influenza virus coupled with intense efforts to control it offer a unique opportunity to document its key epidemiological, virological and pathogenetic properties. This information is crucial for modeling aiming to predict the future burden of disease and to design strategies for most effective control of this pandemic. However, changes to the strain’s properties, including emergence of resistance, would render these predictions invalid. Continued surveillance is therefore of key importance.
Acknowledgements
We thank all health care workers and staff of Municipal Health Services for providing data, and assistance in taking respiratory specimens for laboratory diagnosis.
Dutch New Influenza A(H1N1)v Investigation Team: list of contributors
D Beaujean, T Beersma, C Boucher, M van Boven, P Brandsema, E de Bruin, R Coutinho, C Deuning, F Dijkstra, S Dittrich, T Donker, A van Eijk, R van Gageldonk, S Hahné, P ten Ham, J van der Have, A van den Hoek, W van der Hoek, L Isken, A Jacobi, P Jacobs, M Jonges, H van den Kerkhof, R van Kessel, M Koopmans, A Kroneman, M van der Lubben, A Meijer, J Monen, A Osterhaus, M Petrignani, H Ruijs, M van der Sande, R ter Schegget, M Schutten, M Siebbeles, J van Steenbergen, A Steens, C Swaan, A Timen, H Vennema, L Verhoef, R Vriend, T Waegemaekers, J Wallinga.
References
- Centers for Disease Control and Prevention (CDC). Swine influenza A (H1N1) infection in two children--Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep. 2009;58(15):400-2.
- Centers for Disease Control and Prevention (CDC). Outbreak of swine-origin influenza A (H1N1) virus infection - Mexico, March-April 2009. MMWR Morb Mortal Wkly Rep. 2009 May 8;58(17):467-70.
- World Health Organization (WHO). World now at the start of 2009 influenza pandemic. Statement to the press by WHO Director-General Dr Margaret Chan. 11 June 2009. Available from: http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html
- Commission Decision of 30 April 2009 amending Decision 2002/253/EC laying down case definitions for reporting communicable diseases to the Community network under Decision nr 21/19/98/EC. 2009/363/EC. Official Journal L 110/58. 01.05.2009. Available from: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2009:110:0058:0059:EN:PDF
- Rijksinstituut voor Volksgezondheid en Milieu - Centrum Infectieziektebestrijding (RIVM-CIB), Landelijke Co?rdinatie Infectieziektebestrijding (LCI). Operationeel deeldraaiboek 2. Incidentele introductie nieuw humaan influenzavirus in Nederland [Operational Planning 2. Incidental introduction of new human influenza virus in the Netherlands]. March 2006, updated between May and June 2009. Available from: http://www.rivm.nl/cib/binaries/DB%20Intr%20nieuw%20hum%20influenza%20in%20NL%20juni%2009_tcm92-60133.pdf
- Meijer A, Beerens A, Claas E, Hermans M, de Jong A, Molenkamp R, et al. Preparing the outbreak assistance laboratory network in the Netherlands for the detection of the influenza virus A(H1N1) variant. J Clin Virol 2009;45(3):179-84.
- Tacken M, Mulder J, van den Hoogen H, Tiersma W, Verheij R, Braspenning J. Monitoring Nationaal Programma Grieppreventie 2007 [Monitoring the National Influenza Prevention Programme 2007]. Nijmegen: LINH; 2008. Available from: http://www.nivel.nl/pdf/grieprap%202007-2008.pdf
- Farrington CP. Estimation of vaccine effectiveness using the screening method. Int J Epidemiol. 1993;22(4):742-6.
- Wallinga J, Lipsitch M. How generation intervals shape the relationship between growth rates and reproductive numbers. Proc Biol Sci. 2007;274(1609):599-604.
- Fraser C, Donnelly CA, Cauchemez S, Hanage WP, Van Kerkhove MD, Hollingsworth TD, et al. Pandemic potential of a strain of influenza A (H1N1): early findings. Science 2009;324(5934):1557-61.
- European Centre for Disease Prevention and Control (ECDC). Influenza A(H1N1)v infection. ECDC Situation Report. 8 July 2009. Available from: http://www.ecdc.europa.eu/en/files/pdf/Health_topics/Situation_Report_090708_1700hrs.pdf
- Health Protection Agency and Health Protection Scotland new influenza A(H1N1) investigation teams. Epidemiology of new influenza A(H1N1) in the United Kingdom, April – May 2009. Euro Surveill. 2009;14
See Also:
Latest articles in those days:
- The surveillance programme for avian influenza (AI) in Norwegian wildlife 2025 3 hours ago
- The surveillance programme for avian influenza (AI) in poultry in Norway 2025 3 hours ago
- Emergence of Novel Reassortant H3N2 Avian Influenza Viruses in Southern China: Genetic Complexity and Pathogenicity in Chickens and Mice 3 hours ago
- Pathological evidence of neurotropism and oculotropism in wild black-headed gulls naturally infected with H5N1 high pathogenicity avian influenza 4 hours ago
- Birth cohort effects in adults associated with influenza A(H1N1)pdm09 vaccine effectiveness 16 hours ago
[Go Top] [Close Window]