

Rizzo C, Declich S, Bella A, Caporali MG, Lana S,. Enhanced epidemiological surveillance of influenza A(H1N1)v in Italy. Euro Surveill. 2009;14(27):pii=19266
Background
Following the recent emergence in late April of a new influenza A(H1N1)v virus in the United States and Mexico [1], the same strain has been detected in an increasing number of countries [2,3], and on 11 June the World Health Organization (WHO) officially declared the influenza pandemic. In response to this situation the WHO has recommended enhancing the collection of information on the chain of transmission of the first identified cases in order to timely identify groups of population at higher risk and to guide preventive actions. The information to be gathered is also crucial for validation and refinement of the parameters used in mathematical models to estimate the potential impact of the pandemic. In Italy, the health authorities have developed specific recommendations for epidemiological and virological surveillance [4] based on the WHO and the European Centre for Disease Prevention and Control recommendations [5,6].
The first confirmed cases of influenza A(H1N1)v in Italy were reported in travellers. The preliminary virological findings have previously been described [7]. This report provides the first description of Italian response and main epidemiological findings of the new influenza A (H1N1)v virus infections in Italy.
Methods
A(H1N1)v surveillance
Since 26 April, suspected, probable and confirmed cases of influenza A(H1N1)v virus are to be reported to the Italian Ministry of Health according to the specific European Union case definition [8].
A suspected case is any person meeting the clinical and epidemiological criteria, a probable case is any person meeting the clinical and epidemiological criteria and with a positive laboratory result showing influenza A infection of an unsubtypable type, a confirmed case is any person meeting the laboratory criteria for confirmation [4].
In order to control the spread of the disease, an active surveillance system of individuals presenting with influenza-like illness and recent history of travel to the affected areas has been set up. All individuals coming from affected areas receive specific medical advice through the health authorities at the airports and seaports, in order to refer to the hospital in case of symptoms. Information about demographic data, illness (e.g. date of onset), and type of travel (e.g. flight number or type of cruise ship) has to be collected. Moreover, specific distancing measures (early isolation of cases and precautionary school closure) and antiviral prophylaxis of close contacts of cases have been set up, in order to contain the spread of A(H1N1)v virus in the country. Any person who has been in close contact with a confirmed case is asked to remain at home for 7-10 days avoiding contacts with others.
Local health authorities should notify any suspected, probable or confirmed cases within 12 hours of symptoms onset, to the Ministry of Health (MoH) and to the National Centre for Epidemiology and Health Promotion (CNESPS) at the Italian National Institute of Health (Istituto Superiore di Sanità, ISS) [4].
In Italy, influenza surveillance is routinely based on a nation-wide sentinel surveillance network together with a structured virological surveillance (INFLUNET). The system is based on general practitioners and paediatricians with the aim of monitoring the incidence of influenza-like illness, identifying the extent of the seasonal epidemics and collecting information on circulating strains. Web-based electronic forms are used for data reporting.
Epidemiological investigation of confirmed cases and close contacts
In order to facilitate standardised and timely reporting and updating, the CNESPS in collaboration with the MoH, has developed specific forms for epidemiological investigation of confirmed cases [4] to be recorded on-line. These forms are available at a secure website (https://www.iss.it/Site/FLUFF100/login.aspx). This tool is based on the United Kingdom Avian Influenza Management System (AIMS), which was designed to record, organise and analyse the epidemiological, clinical and personal data for human cases of avian influenza [9], and to facilitate the fulfilment of the International Health Regulations (IHR) requirements.
The information must be collected and entered into the website by the local health authorities within 12 hours after case confirmation. This includes demographic data and details of clinical illness (e.g. date of onset, signs and symptoms, severity, outcome). Data on contacts include exposure data (e.g. relationship to case, type/date of contact, household information) and subsequent development of illness and/or asymptomatic infection. Follow-up information is requested after 15 days from the first epidemiological investigation.
Results
Data from A(H1N1)v surveillance
As of 7 July 2009, a total of 995 suspected cases have been reported to the Italian surveillance system of influenza A(H1N1)v. Of those, 439 (44%) cases were laboratory-tested as negative (excluded), 158 (16%) cases were confirmed and 398 (40%) cases are still under investigation. Of the cases still under investigation 347 had symptoms onset more than one week before 7 July. This indicates that probably only 51 cases can be defined as being still under investigation.
Almost all confirmed cases (n=152) were travel-related, the remaining six cases who acquired the infection in Italy were close contacts of a confirmed travel-associated case. Among the 152 A(H1N1)v cases who had travelled out of the country, 137 (87%) had available data regarding the travel during the week before the date of onset. Of these, 100 (73%) had returned from the United States (US), 8 (6%) had travelled from Mexico, 9 (7%) had been in another European Union Member State, and 14 (10%) had travelled to other countries (Argentina, Canada, Peru, Philippines, and Singapore) (Figure 1). All cases returning from Mexico were reported in the first two weeks of surveillance (24 April - 8 May), and to date, the majority of confirmed cases were travellers to the US.
Figure 1. Distribution of travel-related and locally transmitted confirmed cases of influenza A(H1N1)v in Italy, by date of onset and place of travel, and cumulative number of cases, as of 7 July 2009 (n=138)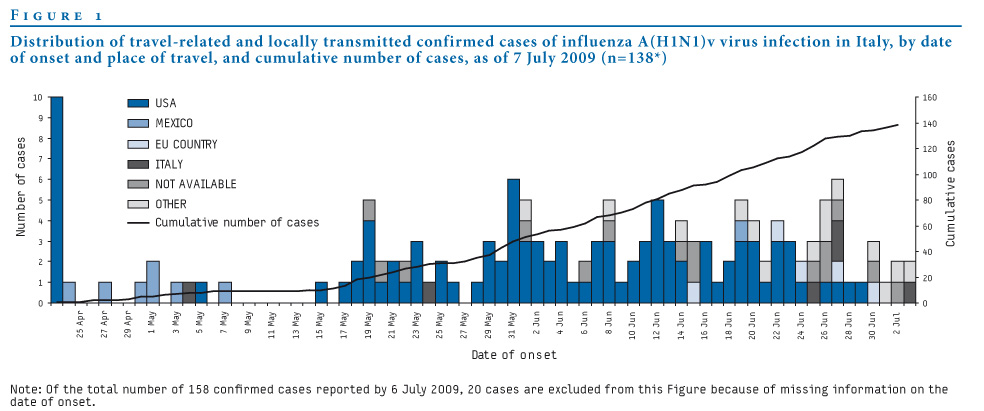
For the 148 (94%) influenza A(H1N1)v cases with available information on age, the median age was 28 years (range 0-69 years) and 83 (56%) were male. Cases younger than 19 years of age constituted 34% of the cases, 59% were aged between 20 and 49 years, and only 7% of cases were 50 years or older (Figure 2).
Figure 2. Distribution by age group and sex of cases of influenza A(H1N1)v reported in Italy, as of 7 July 2009 (n=148)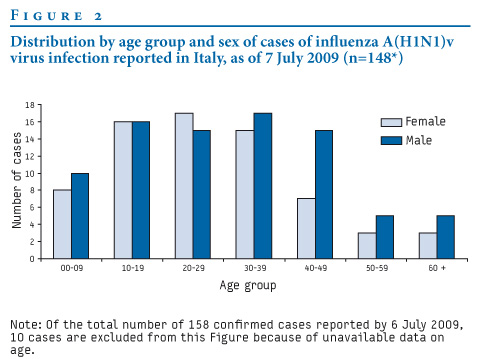
To date, there have not been significant signals of increased influenza activity through the INFLUNET system. Outputs from this system are published on a weekly basis (available in Italian at the website: http://www.iss.it/iflu/).
Data from epidemiological investigation of confirmed cases
Results of the epidemiological investigations of confirmed cases are available for 86 cases. Among these cases, 22 (26%) have been admitted to hospital. It is important to note that some hospitalisations were due to isolation purposes, and therefore the proportion of patients admitted to hospital is not an indicator of the severity of disease. The mean length of stay in hospital was 3.4 days (range 0-7 days). Time elapsed from disease onset to laboratory confirmation was 3.1 day (range 0-12 days). The list of symptoms and the proportion of confirmed cases reporting specific symptoms are given in the Table. Most of the symptoms were reported at disease onset. The most frequent symptoms reported were fever and/or respiratory symptoms, and the least frequent were the gastrointestinal symptoms.
Of the 86 confirmed cases investigated two were healthcare workers. One had travelled abroad, the other one had acquired the infection in Italy due to contact with a confirmed case in hospital setting. Further five confirmed cases were tourists (not Italian residents) travelling on a cruise ship.
Table. Number and proportion of confirmed cases of influenza A(H1N1)v in Italy, reporting specific symptoms, in general and at disease onset (n=86 cases for whom this information was available)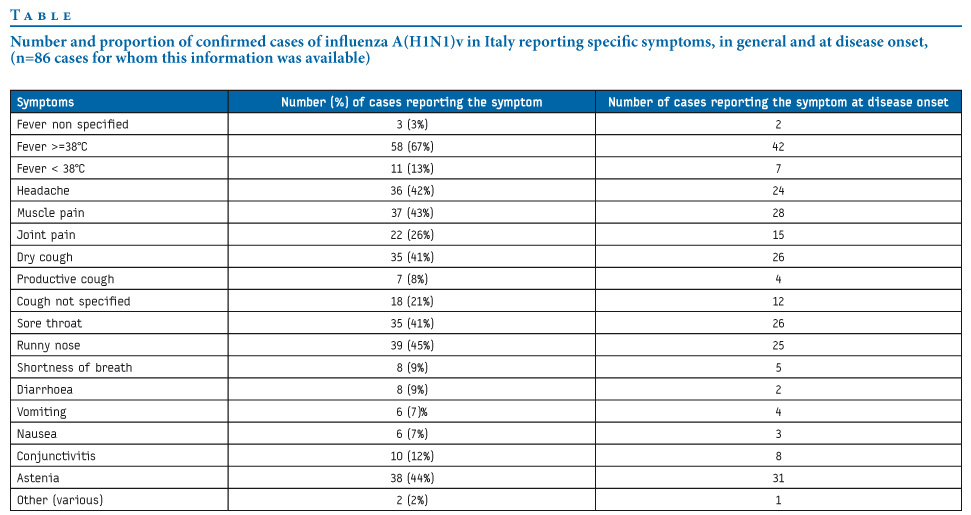
Of the 86 confirmed cases investigated, all received antiviral treatment, once diagnosed, and 90% were treated within 48 hours of symptom onset. Overall 371 close contacts have been identified and put under surveillance, and the average number of contacts for every confirmed case was 5.2 (range 1-39 contacts). Information on prophylaxis of close contacts was available for 319 individuals, 125 of these (39%) received antiviral drugs (114 took oseltamivir, six got zanamivir, and five did not specify the drug taken). Of reported close contacts, 14 (4%) were infected and confirmed as cases, including four who had not received prophylaxis (one because of underlying medical conditions). In 39% of close contacts, antiviral prophylaxis was administered more than 48 hours after symptoms onset of the confirmed case they had been in contact with.
The information on the vaccination status for seasonal influenza in the previous season was available for 73 confirmed cases. The number of persons reported to have been vaccinated during the 2007-8 and 2008-9 seasons was 9 and 2, respectively.
Among 80 confirmed cases for whom information on pre-existing conditions was available, nine persons reported chronic pre-existing conditions (such as cancer, diabetes, heart disease, immunodeficiency conditions). In addition, one case of otitis media in a seven-month-old child and pneumonia in two adults (30 years of age) were reported after the 15 days requested follow-up of cases.
Discussion
The results presented provide some general information on demographic characteristics (age, sex), travel history, clinical presentation, treatment and prophylaxis of patients infected by influenza A(H1N1)v in Italy.
To date, no local sustained transmission has been reported in Italy. Our results should nevertheless be cautiously interpreted, as approximately all confirmed cases were imported from affected areas. Moreover, since 14 May 2009 the number of confirmed cases has been increasing most probably due to the application of specific RRT-PCR test from the US CDC [7] and due to the increasing number of cases worldwide. In particular, in the last week (30 June - 7 July) the number of reported confirmed cases increased from 100 to 158 and the number of close contacts that had been infected and confirmed as cases increased from 4 to 14.
This preliminary description of the current Italian situation highlights that surveillance activities in Italy are effective at this stage of the outbreak for containment purposes. In fact, 90% of confirmed cases received treatment within 48 hours after symptoms onset. However, it should be noted that only 39% of close contacts received prophylaxis. This is probably due to heterogeneity of the use of antiviral prophylaxis because no specific national guidelines are available. No sustained local transmission has been reported to date in Italy (7 July 2009), except for 14 secondary cases.
Epidemiological investigation with the web-based reporting system is crucial in order to gain specific information on pre-existing chronic conditions and complications among hospitalised cases. This data will help to build a comprehensive database in order to better monitor the epidemic in Italy, in particular to identify risk groups and factors contributing to the development of the epidemic. Moreover, this could represent an important opportunity to share data within EU countries using similar approaches [9].
It is clear that this kind of epidemiological investigation cannot be maintained during the epidemic peak when the number of cases becomes too high. However, collecting information on the first few cases, especially those locally transmitted, could be crucial in order to describe the mechanisms of transmission and biological parameters to fill the existing epidemiological gaps.
Acknowledgments
We are grateful to all colleagues from the regional health authorities:
Manuela Di Giacomo and Rossana Cassiani (Regione Abruzzo), Gabriella Cauzzillo and Francesco Locuratolo (Regione Basilicata); Antonio Zaccone (Regione Calabria); Pina Di Lorenzo (Regione Campania); Alba Finarelli, Pierluigi MACINI and Claudio Po (Regione Emilia Romagna); Tolinda Gallo (Regione Friuli Venezia Giulia); Amalia Vitagliano and Pietro Borgia (Regione Lazio); Paola Oreste and Roberto Carloni (Regione Liguria); Anna Pavan and Luigi Macchi (Regione Lombardia); Giuliano Tagliavento, Gualtiero Grilli and Daniel Fiacchini (Regione Marche); D’Alò (Regione Molise); Michela Audenino, Vittorio Demicheli, and Roberto Raso (Regione Piemonte); Cinzia Germinario (Regione Puglia); Rita Masala (Regione Sardegna); Antonella Bullara (Regione Sicilia); Emanuela Balocchini (Regione Toscana); Valter Carraro (P.A. Trento); Maria Donata Giaimo and Anna Tosti (Regione Umbria); Luigi Sudano (Regione Val D’Aosta); Francesca Russo and Giovanna Frison (Regione Veneto).
And to colleagues from the national investigation team, based at the ISS and MoH, who are conducting epidemiological investigations of confirmed cases and are steadily providing data during this period.
References
- Centers for Disease Control and Prevention (CDC). Swine influenza A (H1N1) infection in two children – Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep. 2009;58(15):400-2.
- World Health Organization (WHO). Human infection with new influenza A (H1N1) virus: clinical observations from a school-associated outbreak in Kobe, Japan, May 2009. Wkly Epidemiol Rec. 2009;84(24):237–44.
- European Centre for Disease Prevention and Control (ECDC). ECDC Situation report. Influenza A(H1N1)v infection. Update 22 June 2009. Stockholm: ECDC; 2009. Available from: http://ecdc.europa.eu/en/files/pdf/Health_topics/Situation_Report_090622_1700.pdf
- Ministry of Labour, Health and Social Policy of Italy. Influenza A (H1N1). Azioni del Governo [Actions of the Government]. 2009. [In Italian]. Available from: http://www.ministerosalute.it/dettaglio/approfondimentoFocusNuovo.jsp?id=13&sub=1&lang=it&area=influenzaA
- World Health Organization (WHO). Global Influenza Programme. Global Surveillance during an Influenza Pandemic. Updated draft April 2009. WHO. 2009. Available from: http://www.who.int/csr/disease/swineflu/global_pandemic_influenza_surveilance_apr09.pdf
- European Centre for Disease Prevention and Control (ECDC). Technical report. Surveillance and studies in a pandemic in Europe. June 2009. Stockholm: ECDC; 2009. Available from: http://www.ecdc.europa.eu/en/files/pdf/Health_topics/Surveillance_and_studies_in_a_pandemic_in_Europe.pdf
- Surveillance Group for New Influenza A(H1N1) Virus Investigation in Italy. Virological surveillance of human cases of influenza A(H1N1)v virus in Italy: preliminary results. Euro Surveill. 2009;14(24):pii=19247. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19247
- Commission Decision of 30 April 2009 amending Decision 2002/253/EC laying down case definitions for reporting communicable diseases to the Community network under Decision n° 21/19/98/EC. 2009/363/EC. Official Journal L 110/58. 01.05.2009. Available from: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2009:110:0058:0059:EN:PDF
- McMenamin J, Phin N, Smyth B, Couzens Z, Nguyen-Van-Tam JS. Minimum dataset for confirmed human cases of influenza H5N1. Lancet. 2008;372(9655):2022
See Also:
Latest articles in those days:
- Birth cohort effects in adults associated with influenza A(H1N1)pdm09 vaccine effectiveness 10 hours ago
- Genetic Characterization of Swine Influenza Viruses in Thailand in 2019-2025 Reveals Novel Reassortants 10 hours ago
- Outbreak dynamics of high pathogenicity avian influenza virus H5N1, clade 2.3.4.4b euBB, in black-headed gulls and common terns in Germany in 2023 11 hours ago
- [preprint]The canine respiratory epithelium is a permissive ecosystem for influenza interspecies transmission and emergence 11 hours ago
- [preprint]Explainable and Calibrated AI for Decoding Host-Adaptive Changes in Influenza A Virus 11 hours ago
[Go Top] [Close Window]