Background
In France, in order to detect early influenza A(H1N1)v virus circulation [1], reporting of clusters of at least three cases of respiratory tract infections occurring within one week in a small community without other identified aetiology has been set up [2]. In the early phase of the pandemic, this surveillance was complementary to the national active surveillance of recent travellers from affected areas [3].
On 12 June 2009, the headmaster of a secondary school in the suburb of Toulouse, South Western France, notified 11 absentees among sixth-grade students in the same class that had reported fever and respiratory symptoms. The regional unit of the Institut de Veille Sanitaire and the local health authority requested nasal and throat specimens for viral testing of the three most recent and severe cases among the 11 sick children. On 13 June, two cases were confirmed with influenza A(H1N1)v virus infection.
An investigation was conducted to describe the outbreak and to identify the source of transmission.
Methods
A retrospective cohort study was conducted among all students and staff members of the class in which the first cases were reported. The following case definitions of suspected and confirmed cases were used:
Subsequently, active case finding was initiated among contacts (close family members and social contacts) of all cases (possible, probable or confirmed) of sick pupils of the class. Passive case-finding was also conducted in the whole school by means of posters.
Nasal and throat swabs were taken from all children and staff members of the class: at the school infirmary for asymptomatic children and at the Toulouse regional hospital for symptomatic children. All possible or probable cases identified through subsequent case finding were also investigated at the hospital.
Staff and school children were interviewed face-to-face using a standardised questionnaire. Information on demographics (sex, age), potential exposure to influenza A(H1N1)v virus since 1 June 2009 (personal or close family, travel history, infection in a relative, social gathering) and medical data for symptomatic cases (fever, cough, asthenia, dyspnoea etc.) were collected. The outbreak was described by time and person, and exposure factors were analysed.
Results
The class included 30 students at the age of 11 to 12 years, and 18 staff members had been in contact with the pupils. All students and eight staff members were investigated. We found 20 cases (18 students and two staff members) corresponding to the case definition (five probable cases and 15 confirmed cases). The attack rate was 60% among children and 25% among staff members. Three cases were asymptomatic.
The reported symptoms were headache (94%), cough (88%), fever (76%), asthenia (53%), sore throat (41%) and rhinorrhoea (35%). No complications were reported and no death occurred.
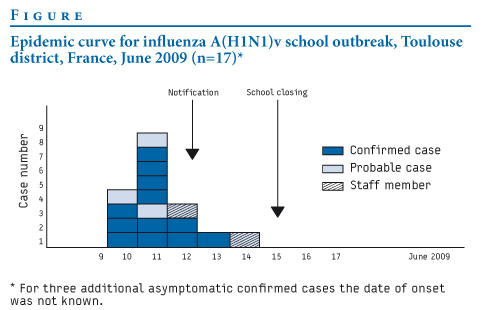
The onset of the outbreak (Figure) among the 17 symptomatic cases was abrupt (10 and 11 June) which could indicate a common exposure to an unrecognised case and secondary transmission from person to person in the following days (12 to 14 June).
Figure. Epidemic curve for influenza A(H1N1)v school outbreak, Toulouse district, France, June 2009 (n=17)*
12 out of 17 (71%) cases corresponded to the definition of a possible case (Table).
Table. Distribution of possible influenza A(H1N1)v cases among students and staff members according to laboratory results, Toulouse district, France, June 2009 (n=38)
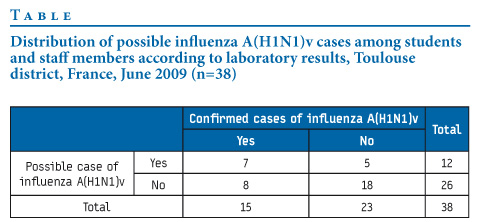
Assuming that a positive real-time PCR was the gold standard, we estimated the sensitivity of the definition of a possible case at 47%, its specificity at 78%, its positive predictive value at 58% and its negative predictive value at 69% among all students and staff members of the class.
In the course of subsequent case finding, nine symptomatic contacts were investigated and only one of them, a student of another class of the school, was confirmed. No case was found among about 120 close family contacts that were traced and among social contacts reported to have had extracurricular activities together with the cases.
None of the students or staff had a history of travelling after 1 June to countries affected by influenza A(H1N1)v or had been in contact with someone symptomatic. However, several children´s relatives worked in sectors related to travel (international firms, airplane construction or air travel staff).
Actions taken
All symptomatic cases were admitted to hospital, examined and treated with antiviral curative treatment (oseltamivir). All close contacts were quarantined and received prophylactic treatment (120 relatives and other social contacts). Each family of a student of the class was interviewed and followed up. The family was asked to call the emergency mobile medical service (Centre 15) if a family member became symptomatic.
On 15 June, the school was closed for one week. The school was reopened on 22 June, since no secondary case had been observed seven days after the last reported case (14 June).
Discussion
This is the first confirmed outbreak of pandemic influenza A(H1N1)v infection reported in France without a well identified chain of transmission. Our investigation could not find any history of travel nor any contact with a previously identified imported case among the children and staff members of this class.
The high attack rate in a single school class, as well as the abrupt onset of the epidemic curve suggests that the children could have shared a strong common exposure. Cases that occurred from 12 to 14 June were probably due to secondary transmission from earlier cases. The fact that no secondary case was observed outside the school after its closure, isolation of cases and prophylaxis of contacts, suggests that these complementary measures were effective to limit transmission to the community.
The source of the outbreak remains unknown. A contact with a previously undiagnosed case could have occurred without being reported. This contact may have occurred within a family, since many parents had occupations related with international travels. Contact with Spanish residents in the area is also possible, related or unrelated with the parents’ occupation. Trade and travels to Spain are frequent in this area of France and the incidence of A(H1N1)v influenza was higher in Spain than in France at the time of the outbreak.
The investigation of the whole school class identified three asymptomatic cases with confirmed influenza A(H1N1)v virus infection. Underreporting of symptoms is unlikely in the context of this intense investigation. Asymptomatic influenza infection is known to occur among about 33% of cases in the seasonal influenza [4]. In a population of 20 cases, we could expect between 12% and 54% of asymptomatic cases, which correspond to our observation (3 of 20 cases).
The low sensitivity (47%) of the French definition of a possible case means that many children had indeed several other symptoms (headache, sore throat, rhinorrhoea, vomiting etc.) than those included in the influenza-like syndrome. This may be due to the high variability of symptoms in children and suggests that this definition was not appropriate for children. In addition, this definition could also be inadequate for adults because the clinical presentation of this new virus was not well-known at the beginning of the outbreak.
Several public health implications arise from this outbreak. After the experience of this cluster, systematic hospitalisation of cases was stopped. Many people in the general population of Toulouse attended newly opened dedicated influenza A(H1N1) consultations, even if they didn’t fulfil the case definition. They were evaluated and none of them was laboratory-confirmed.
This outbreak was an important event that allowed adjusting the surveillance of influenza A(H1N1)v in the early phase that focussed mainly on imported cases. Surveillance is now moving to wide community surveillance through sentinel networks, surveillance of hospitalised severe cases and reporting of clusters.
Acknowledgments
We are grateful to: Jean Claude Desenclos (InVS) for scrutinising the manuscript, Eloi Diène (InVS) and Sophie Larrieu (Cire Aquitaine) for their help in the investigation.
We would like to thank all the people involved in this investigation: children, their parents, and all staff members of the secondary school, clinicians from the regional hospital and the regional laboratory (CHU Purpan, Toulouse), colleagues from Toulouse local health departments and school medical services.